How the orthopaedic unit was created
Kevin King: Head of first orthopaedic unit at Footscray Hospital from 1964–1985
“The first thing I did was get control of my own patient admissions. Before that the admissions were done by someone down in the admissions office. I wasn’t having any of that because only the surgeons running the unit know which patients are the right priority.
If you’re going to run a proper unit and you’re well motivated in doing the best for the patients, you’ve got to get control of your admissions. So you have a balance of perhaps two total hips, two knees, plus one or two arthroscopies. It’s a matter of common sense.
You then must have an efficient ward. I’ve always regarded the ward sister – the senior charge nurse - as the most important person in the public hospital system.
I then got a splendid number two, Jonathan Rush and Jonathan and I ran the unit by ourselves for about five years. By that stage the unit rapidly expanded and we had new wards built.
We managed to get most of what we wanted from the hospital’s board. It was an extremely sympathetic board. It was a working class board, of whom the chairmen were always tough, wealthy people of working class origins. And if you went to see them with a good case, they’d listen.
For example the Lions Club bought us the latest internal fixation equipment used for fractures, worth many thousands of dollars. In those days, that was big money.
We always got access to the latest radiology and internal fixation equipment, reinforced always by Sister McNeilage’s opinion.
In the 70s we were one of the first units to get the first mobile imagine intensifier, which revolutionised, from an orthopaedic view, the internal fixation of long bone fractures in the lower limbs.”
Milestones in surgery
In the 1930s Kevin King’s father, Tom King, an orthopaedic surgeon at St Vincent’s hospital, pioneered a technique of pinning the hips of patients who had a fractured neck of femur, (thigh bone) one of the most common of all fractures.
“Before my father developed this technique many of these patients died because they developed bed sores and they weren’t internally fixed. My father Tom King invented a technique where you put a pin through the skin, using x-ray machines which had separate films.
The later image intensification fracture system introduced in the 1970s was basically the same system – but much quicker and less cumbersome. It too involved inserting pins internally and fixing fractures with minimal trauma.
Polio was an interesting disease from the point of an orthopaedic surgeon because you could plan out the weaknesses and paralysis. You could take a child and do a series of seven operations over two years and give them 70 per cent of the mobility they once had.
You could take a child who had been in a wheelchair and plan operations, fuse joints and switch tendons around. Now that’s all gone, thank God, because polio was a terrible scourge.”
Other breakthroughs
“Sepsis has always been the curse of orthopaedics. So the major breakthrough in my generation of surgeons was the combination of antibiotics and joint replacement.
Joint replacement is a first class operation because of its ability to produce so much pain relief. No major operation in orthopaedics has ever worked so well, apart form the original internal fixation of fractures by the pinning technique of the hips.
Other breakthroughs included the image intensifier, which cut radiation dosages down to a safe degree for patients.
When I was a registrar in England there were 10 different sets of internal fixation equipment – all of different metals and different shapes and sizes. There was one for the radius, (forearm bone) one for the humerus, (the long bone in the upper arm) and so on. That was hopeless. So from the 1970s onwards the Swiss mechanised the process.
Professor Maurice Muller, who was professor of orthopaedics in Berne industrialised the process by producing an entire integrated system of internal fixation devices.
It meant you could internally fix any fracture in the body with the same system. It was a marvellous advance. The devices –plates and screws etcetera - were all standardised and interchangeable. That greatly increased the range of safe internal fixation of major fractures.
Arthroscopy was also a major advance. Arthroscopy did for joints what the image intensifier did for other parts of fractures. It enabled you to do things that you would otherwise have to make a large incision for.
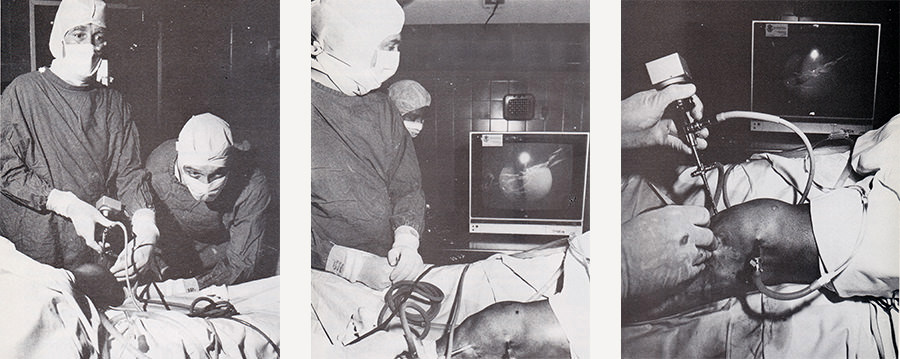
Orthopaedic surgeons perform knee joint surgery in 1985 using an arthroscope. The Lions Club of Footscray raised $20,00 to buy new arthroscopic equipment for the team.
Western Health archives
The orthopaedic training scheme was the first of the surgical training schemes in Australia. It started in 1968 - 20 years before they introduced equivalent training programs in the UK.”
(Mr King was involved in the College of Surgeons’ orthopaedic training program until he retired)
A legacy
“By the time I left Footscray there were about five orthopaedic surgeons in the unit. The Board allowed us to have about 20 per cent of private patients in the wards provided the chaps did their 80 per cent of public work. By that stage they were all on sessional payments. I found that a much better system for running a department. Footscray’s orthopaedic unit was as busy as the Royal Melbourne’s.”

